Robust evidence demonstrates the benefits of prompt AVR in patients with severe aortic stenosis (AS)1-5
In a real-world meta-analysis of over 1400 asymptomatic severe AS patients2:
Early AVR in patients prior to symptom onset significantly reduced rates of stroke (pooled rate 4.5% vs 7.2%; HR: 0.62; 95% CI: 0.40-0.97; I2=0%; P=0.03)2
TAVR by Edwards is approved for severe AS patients regardless of symptoms
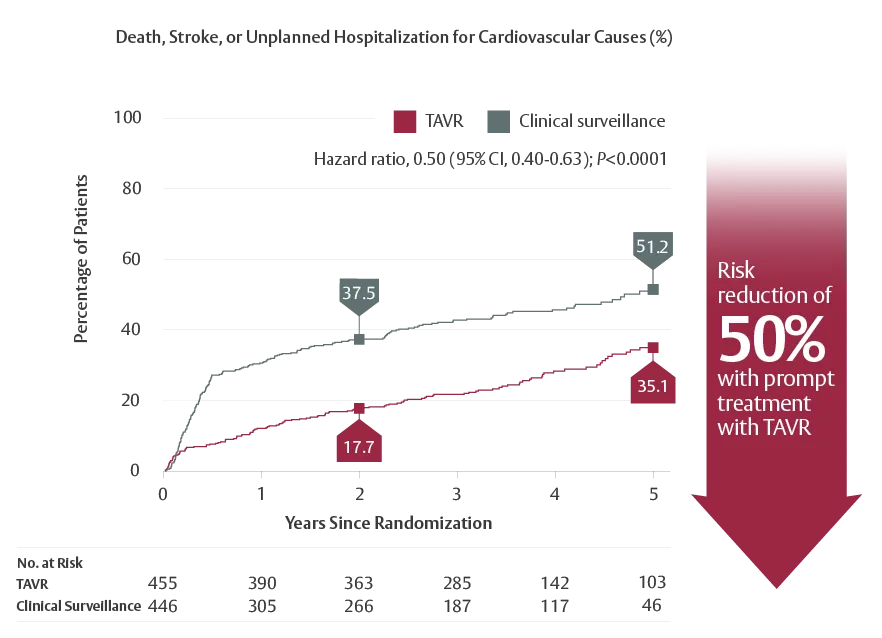
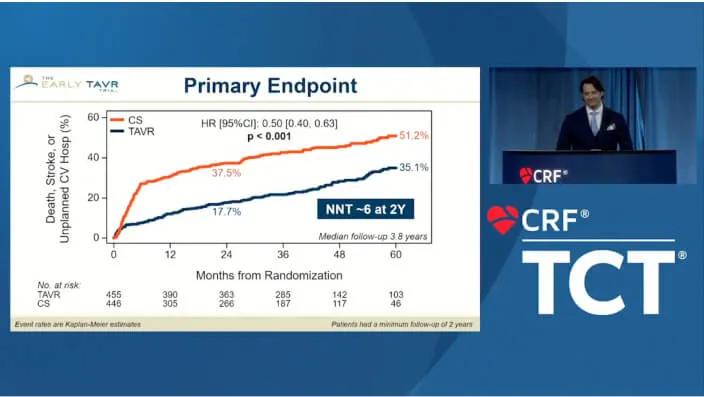
The EARLY TAVR trial proved that prompt intervention with TAVR by Edwards was superior to clinical surveillance in the primary composite endpoint of death, stroke, or unplanned cardiovascular hospitalization* in asymptomatic severe AS patients†1
Primary composite endpoint at 5 years†1:
*Including any aortic valve intervention or reintervention within 6 months.1
†
The EARLY TAVR trial is a prospective, multicenter RCT that compared early TAVR (SAPIEN 3/SAPIEN 3 Ultra) to guideline-recommended clinical surveillance among patients with asymptomatic severe AS. The primary endpoint was a composite of death, stroke, or unplanned cardiovascular hospitalization. Unplanned cardiovascular hospitalization includes any aortic valve intervention or reintervention within 6 months. Secondary endpoints included favorable health status outcome.1
There’s significant risk to watchful waiting for patients with severe AS1
Even careful surveillance is twice as likely to result in unexpected or emergency cardiovascular hospitalization‡ than receiving early treatment1
Prompt TAVR resulted in a 68% lower risk of hospitalization for heart failure through 5 years vs clinical surveillance (5.3% vs 12%)§1
‡Includes any unplanned cardiovascular hospitalization and any aortic valve intervention or reintervention within 6 months.1
§KM estimate at 5 years.1
TAVR for Asymptomatic Severe Aortic Stenosis: Results of the EARLY TAVR Trial
For more details on the outcomes of the EARLY TAVR trial, use this link to access the New England Journal of Medicine publication. No registration is necessary.
New England Journal of Medicine Transcatheter Aortic-Valve Replacement for Asymptomatic Severe Aortic Stenosis
Reintervention rates are exceedingly low with TAVR—over 98% of patients did not require valve reintervention after 10 years7
TAVR by Edwards demonstrates excellent structural integrity in accelerated wear testing; an equivalent of 25 years of wear with no differences compared to surgical valves8
Paravalvular leak (PVL) contributes to valve deterioration. The Edwards SAPIEN 3 Ultra valve demonstrated excellent PVL performance with 87% experiencing no/trace PVL at 30 days9,10
READY TO HAVE THE TAVR DISCUSSION WITH YOUR PATIENT?
Download the TAVR Info Kit, which contains details about the procedure.
The EARLY TAVR TrialTM is a prospective, multicenter RCT that compared early TAVR (SAPIEN 3/SAPIEN 3 Ultra) to guideline-indicated clinical surveillance among patients with asymptomatic severe AS. The primary endpoint was a composite of death, stroke, or unplanned cardiovascular hospitalization. Cardiovascular hospitalization includes aortic valve intervention within 6 months of randomization (clinical surveillance arm) or aortic valve reintervention within 6 months of the study procedure (TAVR arm). Secondary endpoints included favorable health status outcome.
†
SAPIEN 3 TAVR was studied in the PARTNER 3 Trial. The PARTNER 3 Trial, SAPIEN 3 TAVR was proven superior to surgery on the primary endpoint of all-cause death, all stroke, and re-hospitalization (valve-related or procedure-related and including heart failure) at one year, and multiple pre-specified secondary endpoints in low risk patients.
‡
PARTNER 3 Trial 5-Year Results in low-risk patients—Low rates of cardiovascular mortality through five years (5.5% SAPIEN 3 TAVR to 5.1% SAVR). Low rates of all-cause mortality through five years (10.1% SAPIEN 3 TAVR vs. 8.2% with SAVR). Low rates of disabling stroke through five years (2.9% SAPIEN 3 TAVR to 2.7% SAVR). Low rates of stroke through five years (5.8% SAPIEN 3 TAVR vs. 6.4% SAVR). Lower rates of rehospitalization with SAPIEN 3 TAVR through five years (13.7% vs. 17.4%).
§Incorporates all commercially available valves at the time of analysis.
SAPIEN 3 Transcatheter Heart Valve System and SAPIEN 3 Ultra TAVR involve serious risks, including death, stroke, major bleeding, and major vascular complications.
References:1.Généreux P, Schwartz A, Oldemeyer JB, et al. Transcatheter aortic-valve replacement for asymptomatic severe aortic stenosis. N Engl J Med. 2025;392(3):217-227.2.Généreux P, Banovic M, Kang DH, et al. Aortic valve replacement vs clinical surveillance in asymptomatic severe aortic stenosis: a systematic review and meta-analysis. J Am Coll Cardiol. 2025;85(9):912-922.3.Otto CM. Timing of aortic valve surgery. Heart. 2000;84(2):211-218. 4.Treibel TA, Kozor R, Schofield R, et al. Reverse myocardial remodeling following valve replacement in patients with aortic stenosis. J Am Coll Cardiol. 2018;71(8):860-871. 5.Malaisrie SC, McDonald E, Kruse J, et al. Mortality while waiting for aortic valve replacement. Ann Thorac Surg. 2014;98(5):1564-1571.6.Mack MJ, Leon MB, Thourani VH, et al. Transcatheter aortic-valve replacement in low-risk patients at five years. N Engl J Med. 2023;389(21):1949-1960.7.Baron SJ, Ryan MP, Chikermane SG, Thompson C, Clancy S, Gunnarsson CL. Long-term risk of reintervention after transcatheter aortic valve replacement. Am Heart J. 2024;267:44-51.8.Sathananthan J, Hensey M, Landes U, et al. Long-term durability of transcatheter heart valves: insights from bench testing to 25 years. JACC Cardiovasc Interv. 2020;13(2):235-249.9.Généreux P, Piazza N, Alu MC, et al. Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research. Eur Heart J. 2021;42(19):1825-1857.10.Nazif TM, Cahill TJ, Daniels D, et al. Real-world experience with the SAPIEN 3 Ultra transcatheter heart valve: a propensity-matched analysis from the United States. Circ Cardiovasc Interv. 2021;14(9):e010543.
Patients and/or clinicians quoted on this website have received compensation from Edwards Lifesciences.
You are about to leave TreatHeartValveFailure.com
By clicking this link, you understand that the website that you will be taken to is not controlled or endorsed by Edwards Lifesciences (“Edwards”), and Edwards does not own, control or influence the content found on the third-party website. You also understand that Edwards does not own or control any first- or third-party advertising, marketing or analytics technologies that may be on the third-party website.
TAVR by Edwards is now the FIRST and ONLY TAVR to be approved for the treatment of both symptomatic and asymptomatic patients with severe aortic stenosis, also known as heart valve failure.